



INTRODUCTION.
Colorectal cancer (CRC) is one of the main problems in modern clinical oncology. The analysis of the recent available publications revealed a tendency towards an increase in the morbidity rate of colorectal cancer worldwide [1; 2]. Annually, more than 1,200,000 patients are diagnosed with colorectal cancer and 639,000 cases of lethal outcomes are registered because of the disease progressing. The statistics on the oncologic morbidity says that colorectal cancer occupies one of the leading places in the rank of oncological diseases in the economically developed countries (10-15% from the total amount of cancer patients) [3; 4]. This pathology occupies the third place in the structure of the morbidity and the second place in the structure of lethality from oncologic diseases in the majority of the developed countries, including Russia [5; 6]. Annually, the morbidity rate increases by 2.3% and the lethality rate – by 3.4% [7]. It is expected that in the first part of the 21st century, colorectal cancer will take the leading place in the structure of oncologic diseases [8].
Surgical treatment for colorectal cancer is the main component of modern effective therapy and the only method of radical resection of the tumor [9; 10].
Presently, the rate of planned surgeries for CLC in older and senior patients with comorbid pathology is increasing [11; 12]. It is associated with the development of medical technologies and the demographic process of population aging. According to the experts from the International Society of Geriatric Oncology (SIOG), the often unsatisfactory outcome of the treatment of this group of patients is observed because of non-optimal evaluation of perioperative risks in patients with comorbid diseases [13; 14]. The outcomes of surgical treatment in older and senior patients with CLC are comparable with the outcomes in patients younger than 60 years old in the case of timely and adequately compensated nonsurgical nosologies.
A high rate of lethality within the 1st year after the diagnostics of CLC is explained by the fact that the primary tumor is diagnosed at later stages (3rd-4th stages) in more than 70% of patients with colon cancer and 60% of patients with rectal cancer. Only 40% of these cases are surgically curable [15; 16]. There are still attempts to search for a simple, universal, and reliable parameter that would allow for the screening evaluation of the possibility of the development of cardiovascular complications during non-cardiac surgical interventions. There is a method of predicting cardiovascular complications in the early postoperative period by the analysis of anamnestic, clinical-instrumental, and laboratory risk factors using such scales as APACHE II, III, SOFA, SAPS I, II, MODS, etc. Besides, additional characteristics of the comorbid status are used, in particular, the modified Charlson index, ICED (Index of Co-Existent Disease), etc. [17].
In the majority of cases, the mentioned scales and indexes do not have precise quantitative criteria and do not take into account the peculiarities of age-related norms of functional parameters, especially, in patients from older age groups, which does not always provide adequate prognosis of the development of acute left ventricular failure in the early postoperative period. Thus, the development and implementation of additional echocardiographic criteria in the clinical practice, in particular, the Tei index, contributing to the increase in the precision of prognosis of possible acute left ventricular failure in patients that underwent surgical treatment for CLC, is quite promising. This approach in cardiologic practice is relatively simple, non-invasive, informative, and highly-efficient for the evaluation of hidden hemodynamic disorders that allows for the effective prognosis of postoperative cardiovascular complications.
The study was aimed to improve the results of surgical treatment for colorectal cancer in older and senior patients using the proposed algorithm of perioperative observation of patients with a high operative-anesthesiological risk.
MATERIALS AND METHODS
The analysis of the results of the examination and surgical treatment of 172 patients with CLC was performed. The study included patients aged 61 to 96 years old. All patients were divided into two groups. The main group included 86 patients aged 75.1+8.0 years old. In this group, an extended algorithm of perioperative observation of patients was used, wherein the cohort was evaluated by specialists from a multidisciplinary team that included a cardiologist and a specialist on functional diagnostics, with the further calculation of the Tei index. The control group included 86 patients aged 75.6+8.4 years old. In this group, the authors did not apply the proposed algorithm of diagnostics. The main group included 45 men and 41 women. The control group included 33 men and 53 women. In general, the share of men in these groups was 45.3% and the share of women was 54.7%. By the age group, patients were divided into older (61-75 years old) – 96 patients, senior (76-90 years old) – 69 patients, and long-living (90 years old and older) – 7 patients (Table 1).
Table 1
Distribution of the examined patients by age groups
|
Age groups (years) |
Groups |
Total |
||||
|
Main |
Control |
|||||
|
Abs. |
% |
Abs. |
% |
Abs. |
% |
|
|
61-75 |
48 |
55.8 |
43 |
50.0 |
91 |
52.9 |
|
76-90 |
35 |
40.7 |
34 |
39.5 |
69 |
40.1 |
|
90 and older |
3 |
3.5 |
4 |
4.7 |
7 |
4.1 |
|
Total |
86 |
100.0 |
86 |
100.0 |
172 |
100.0 |
All patients from the main and control groups had a polycomorbid background (Table 2). On average, one patient had two and more diseases and was characterized by a high operative-anesthesiological risk by the scale of the Moscow Scientific Society of Anesthesiologists-Reanimatologists (MSSAR) (7.1+1.1 and 6.7+1.1 points, respectively).
Table 2
The rate of comorbid pathology in patients from the studied groups
|
Comorbid pathology |
Control group |
Main group |
|
Stable effort angina |
44 (51.2%) |
32 (37.2%) |
|
Atherosclerotic cardiosclerosis |
80 (93.0%) |
82 (95.3%) |
|
Postinfarction cardiosclerosis |
23 (26.7%) |
10 (11.6%) |
|
Hypertensive disease of the 1st-3rd degree |
86 (100%) |
86 (100%) |
|
Chronic heart failure |
47 (54.7) |
36 (41.9%) |
|
Acute cerebrovascular event in the anamnesis |
15 (17.4%) |
12 (13.9%) |
By the localization of the tumor, patients were divided into two groups: a malignant tumor of the rectosigmoid junction was diagnosed in 54.6% of patients from the main group and a malignant tumor of the rectum was diagnosed in 60.5% of patients from the main group.
Among the clinical peculiarities of patients from both groups, abdominal syndrome prevailed. In 109 patients from both groups, it was subjectively evaluated as the “most significant”. At the same time, the pain itself, its localization, character, and intensity were different. Cramp-like pains prevailed in the main (59.0%) and control (50.1%) groups.
The instrumental part of the clinical-functional study additionally included the calculation of the Tei index. During the echocardiographic study, transthoracic apical access in the 5-chamber section was used in the mode of continuous-wave Doppler with simultaneous registration of transmitral and transaortic flows. The myocardial index (Tei index) was calculated as a sum of periods of isovolumetric contraction (IVCT) and isovolumetric relaxation (IVRT) divided by the ejection time (ET) by the formula: Tei= (IVCT+IVRT)/ET. Normally, the Tei index for the left ventricle was 0.36 ± 0.04. This parameter was evaluated in the preoperative period, on Day 1, and Days 10-11 after the surgery. These are the generally accepted endpoints that include potentially unfavorable clinical periods of condition worsening in patients with the development of cardiovascular complications.
When the Tei index of cardiac dysfunction was higher than 0.79, patients had clinically-instrumental predictors of left ventricular heart failure diagnosed. The specified Tei index indicated an increase in the length of the systolic period in the cardiac cycle, which decreased the efficiency of the left ventricle contraction being a potential cause of the development of the left ventricle heart failure. Patients with such values of the Tei index were classified as the risk group. Further cardiotropic pharmacological correction prevented possible cardiovascular complications.
Statistical analysis of the obtained results was performed with the software package STATISTICA for Windows (ver. 7). The comparison of frequency characteristics (sex, complications, comorbid pathology) was made using non-parametric Yates tests (for small groups) and the Fisher test.
The study protocol followed guidelines for experimental investigation with human subjects in accordance with the Declaration of Helsinki and was approved by the ethics committee. Written informed consent was obtained from each patient (or an official representative) before the study.
RESULTS
After the realization of the generally accepted standard preoperative diagnostic algorithm that included laboratory (clinical blood assay, biochemical blood assay, tests for hepatitis, HIV and syphilis, blood group and rhesus factor, common urine test) and functional methods of study (ECG, chest X-ray and abdominal USI), all patients from the main group had the Tei index calculated additionally. Before the surgery, 27 out of 86 patients had the Tei index higher than the reference (0.41 to 0.89). This difference in values required a differentiated approach to the correction of possible cardiovascular complications. The threshold index value that reflected the risk of the development of acute left ventricular heart failure in the early postoperative period (Day 1) was 0.79. Such an increase in the Tei index was registered in 16 patients. It should be noted that the most often clinical manifestations associated with a significant increase in the Tei index value were hypertensive conditions (67%), myocardial ischemia (52%) or their combination (38%). The performed pathogenetic cardiotropic therapy compensated the mentioned alterations and, on Days 10-11 after the surgery, the Tei index was higher than 0.41 only in 4 patients. The specified data is presented in Table 3.
Table 3
Dynamics of the Tei index in patients from the main group in the postoperative period
|
Period |
Tei-index |
|
|
0.36 ± 0.04 |
0.41-0.89 |
|
|
Before the surgery |
59 |
27 |
|
On Day 1 |
70 |
16 |
|
On Days 10-11 |
82 |
4 |
Based on the data obtained in patients from the group of high risk, additional preventive cardiotropic pharmacologic correction was performed during the postoperative treatment that was indicated by the results of the monitoring of the Tei index on Day 1 and Days 10-11 after the surgery.
Thus, patients from the main group had a significant advantage in the prevention of the risk of the development of cardiovascular complications in the postoperative period over the control group. In further, this allowed the surgeons to expand the operability and increase the number of radical resections (Table 4).
Table 4
Structure of the performed surgical intervention
|
Outcome |
Control group |
Main group |
Total |
|
Abdominoperineal extirpation |
13 (15.12%) |
50 (58.14%) |
63 |
|
Anterior resection |
12 (13.95%) |
17 (19.77%) |
29 |
|
Hartmann’s operation |
16 (18.6%) |
14 (16.28%) |
30 |
|
Stoma exteriorization |
43 (50.0%) |
5 (5.81%) |
48 |
|
Other |
2 (2.33%) |
0 |
2 |
The analysis of the number of postoperative complications in both groups using the method of prognosis of early postoperative cardiovascular complications in patients that underwent radical surgical treatment for colorectal cancer (92 patients: 67 patients from the main group, 25 patients from the control group) showed that the highest rate of complications was observed in the control group (12.0%) (11 patients) and in the main group (7.6%) (7 patients). The specified data is presented in Table 5.
Table 5
Postoperative cardiovascular complications in patients that underwent radical resection (n=92)
|
Outcome |
Control group (n=25) |
Main group (n=67) |
|
Acute myocardial infarction (AMI) |
4 (16.0%) |
2 (2.9%) |
|
Pulmonary artery thromboembolism (PATE) |
2 (8.0%) |
1 (1.5%) |
|
Heart rhythm disorder |
3 (12.0%) |
2 (2.9%) |
|
Congestive heart failure |
2 (8.0%) |
2 (2.9%) |
The comparative analysis in both groups revealed that the leading place in the structure of surgical complications is occupied by septic-inflammatory complications in the surgical site, in particular, suppuration on the laparotomy wound side in the main group in 3 (3.5%) patients and in the control group in 5 patients (5.8%), which was associated with Hartmann’s operation and colostomy exteriorization. In the area of the perineal wound in the main group, seroma of the blind suture was observed in 3 patients (3.5%) and suppuration in the perineal area – in 4 patients (4.7%) after the tamponing of the presacral space. The second place by the rate of occurrence was occupied by an intraabdominal hemorrhage. In patients from the main group, it was observed in 2.3% cases (2 patients) (anterior resection and abdominoperineal extirpation). In the control group, there were 4.7% of such cases (4 patients), 2 of them (anterior resection) underwent relaparotomy. The structure of postoperative complications also included early adhesive obstruction. Each group contained 1 patient (1.2%) that had to underwent treatment for early adhesive small bowel obstruction. Both patients underwent relaparotomy. In the rest 77 patients (89.5%) from the main group and in 72 patients (83.6%) from the control group, the postoperative period was uncomplicated (Figure 1).
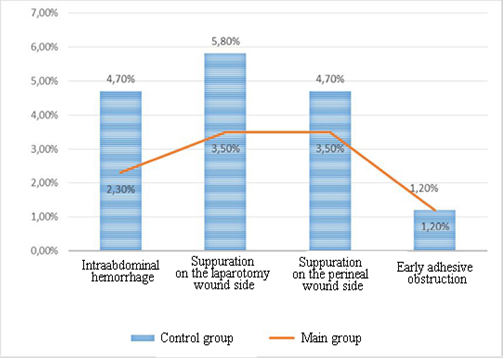
Fige 1. Postoperative surgical site complications
The postoperative lethality in all the operated patients (n=172) was 5.8% (5 patients) in the main group and 25.5% (22 patients) in the control group.
A comparative analysis of the causes of the lethal outcome in patients from both groups (n=172) showed that multiple organ failure had the highest rate. In the control group, it was 11.6% (10 people) and in the main group, it was 3.5% (3 people). Four out of ten patients from the control group had anterior resection of the rectum, one – abdominoperineal extirpation, and five – sigmostoma exteriorization as a palliative method of treatment. Three patients from the main group had a different volume of surgical treatment. One patient had anterior resection of the rectum, the second – Hartmann operation, and the third – sigmostoma exteriorization. These three patients were operated for upper and middle ampullary rectal cancer. Despite the performed pharmacological therapy and prevention of cardiovascular complications, in the postoperative period, there were lethal cases caused by acute myocardial infarction and pulmonary artery thromboembolism: 1 and 1 patient (1.3%) in the main group and 5 (5.8%) and 7 patients (8.1%) in the control group (Table 6).
Table 6
Causes of lethal outcome in the studied groups
|
Causes of lethal outcome |
Control group (n=86) |
Main group (n=86) |
|
Multiple organ failure |
10 (11.6%) |
3 (3.5%) |
|
AMI |
5 (5.8%) |
1 (1.2%) |
|
PATE |
7 (8.1%) |
1 (1.2%) |
CONCLUSIONS.
A multidisciplinary approach that involves additional functional-diagnostic and instrumental methods, in particular, Doppler echocardiography with the calculation of the Tei index, allows for the prognosis of early left ventricular heart failure in the postoperative period. This provides a possibility to optimize surgical treatment of colorectal cancer in older patients with a polycomorbid background, compensate cardiovascular risk, increase the operability, and decrease the rate of postoperative complications.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
The authors declare no conflict of interest