


Aims
The aim of the study was the development and clinical approbation of the method of treatment of purulent arthritis with the formation of ankle ankylosis.
Materials and Methods
Twenty-two patients underwent surgery after ankle trauma complicated by inflammation (18 male and 4 females ranging in age from 28 to 62). To open the ankle joint, an anterior approach was used. After opening the cavity of the joint, surgical treatment of the purulent-necrotic focus with necrotic sequestrectomy and resection of the tibia and talus bones were performed within the limits of healthy bone tissue, after which a compression/distraction device was applied. Distraction in the area of the resection of the tibia and talus bones artificially created a cavity in the ankle joint simultaneously. Through additional punctures in the projection of external and internal ankle bones, a perforated drain was placed in the created cavity. [Bonesaw-lines] of the tibia and talus bones were drawn together to the dimensions of the drain tube. In the postoperative period, sanitation of the purulent-necrotic focus was performed by means of continuous draining of the created cavity with antiseptic solutions. After the bacterial inoculation cultures were negative three times, the draining tube was removed, and gradually the tibia and talus bones were moved closer. The external fixation device was switched to the mode of consistent stabilisation with the possibility of putting weight on the damaged extremity. Fixation in the device continued until the X-ray picture of bone ankylosis in the ankle was obtained
Results
For all patients we were able to achieve stable remission of the inflammation process and formation of a strong bone ankylosis in the ankle. The sanitation period of the purulent-necrotic focus was 14–16 days. After removal of the drain and compression in the external fixation device, the patients were allowed to move on crutches with moderate weight on the operated extremity. Duration of fixation in the device was 16–20 weeks. During 5 years of continuous follow-up, no relapses of inflammation in the ankle joint were observed.
Conclusions
The suggested method makes it possible to solve the problem of ending inflammation in the ankle by means of forming bone ankylosis during surgical treatment of purulent osteoarthritis.

- Pankov I.O., Emelin A.L., Nagmatullin V.R. Transosseous osteosynthesis in supinal inversion fractures of distal articular tibia [Chreskostnyi osteosintez pri supinatsionno-inversionnykh perelomakh distal'nogo sustavnogo otdela kostei goleni]. Practical Medecine - Prakticheskaia meditsina, 2013, vol. 69, no. 1-2, pp. 114-118.
- Korzh N.A., Bets G.V., Bets V.G. Role of therapeutic immobilization in prevention of infectious complications in case of open ankle joint injuries [Rol' lechebnoi immobilizatsii v profilaktike infektsionnykh oslozhnenii pri otkrytykh povrezhdeniiakh golenostopnogo sustava]. Trauma - Travma, 2007, vol. 8, no. 3, pp. 343-348.
- Shchad'ko A.A. Individual reconstructive and restorative approach to treatment of patients with purulent ankle arthritis [Individual'nyi rekonstruktivno-vosstanovitel'nyi podkhod k lecheniiu bol'nykh s gnoinymi artritami golenostopnogo sustava]. Ukrainian Journal of Surgery - Ukrainskii zhurnal khirurgii, 2013, vol. 20, no. 1, pp. 65-68.
- Korolev R.S. The treatment of purulent osteoarthritis of the ankle joint with compression arthrodesis [Lechenie gnoinykh osteoartritov golenostopnogo sustava pri pomoshchi kompressionnogo artrodeza]. IX Congress of Orthopaedic Traumatologists: Collection of theses [IX s"ezd travmatol.-ortopedov: sb. tezisov], Saratov, 2010, p. 423.
- Barabash Iu.A., Barabash A.P., Grazhdanov K.A. Method of ankle arthrodesis in purulent osteoarthritis. Patent of the Russian Federation [Sposob artrodeza golenostopnogo sustava pri gnoinykh osteoartritakh. Patent Rossiiskoi Federatsii], № 2435541, 10.12.2011.
- Barabash A.P., Norkin I.A., Barabash Iu.A. Atlas of perfect osteosynthesis of diafysical fractures of tibia bones [Atlas ideal'nogo osteosinteza diafizarnykh perelomov kostei goleni]. Saratov, Oformitel', 2009, 64 p.
INTRODUCTION.
Presently, the damage of distal ankle bones is the most common type of injury. Their rate reaches 20-40% of all lower limb fractures [1]. It is not always possible to extend the indications for osteosynthesis, which inevitably leads to an increase in the rate of post-operative complications characterized by an inflammation in the joint cavity. Often, septic inflammation of the ankle joint develops after open fractures of ankles, gunshot wounds or as a secondary complication in patients with osteomyelitis of the inferior metaepiphysis of the tibia, astragalus or calcaneus bones [2]. The treatment of post-traumatic septic arthritis is an acute problem in modern traumatology. According to the published data, the share of septic infections in the ankle joint is about 38.5% of all the septic-inflammatory pathologies of major joints [3]. The peculiarities of the structure of the ankle joint contribute to the quick onset and severe development of the inflammatory process. Septic infection in the ankle joint is characterized by persistent development and frequent recurrences. Major difficulties in the treatment are caused by a deficit of soft tissues, their trophic alterations, and high bacterial content on the skin. Often, a conventional treatment that includes joint punctures and antibacterial therapy is unsatisfactory. For this reason, active surgical sanitation in the treatment of septic arthritis of the ankle joints a priority [4].
An important element in the treatment of the septic-necrotic process is active drainage of the inflammation foci. Due to the peculiarities of this anatomic structure, the drainage of the ankle joint is almost impossible, only astragalectomy can provide favorable conditions for the drainage of the joint. The proposed method of surgical treatment of septic arthritis of the ankle joint includes artificial creation of a cavity in the joint and its active sanitation with further compression of the two joint surfaces of the astragalus and tibia by external fixation.
The study was aimed to develop and clinically test a new technology of the treatment of septic arthritis with the formation of bone ankylosis of the ankle joint.
MATERIALS AND METHODS
The clinical group of observation included 22 patients with ankle joint injuries complicated by an inflammatory process that underwent treatment from 2010 to 2016 at the Department of Septic Surgery of the Scientific Research Institute of Traumatology, Orthopedics and Neurosurgery. The clinical group included 18 men and 4 women aged 28-62 years old.
The present study was approved by the local ethical committee. The aim and methods were explained to the participants who signed the form of the informed consent for the examination, treatment, and publication of the obtained data.
The pre-operative period included the clinical examination of patients, evaluation of the degree of involvement of soft tissues in the inflammatory process, laboratory diagnostics (general blood assay, the biochemistry of blood and coagulogram), X-ray imaging of the injured ankle joint for the evaluation of the degree of the damage of bone structures. Computed tomography was performed for the specification of the spatial position of the bone structures that form the ankle joint, evaluation of the involvement of astragalus and tibia into the inflammation process, and identification of septic pockets. Patients with synovial fistula underwent a contrasting study. For the evaluation of the sensitivity of pathogen microflora to antibiotics and indication of rational antibiotic therapy in the post-operative period, the bacteriological study of the synovial fistula discharge (or punctate of the ankle joint) was performed.
The technique of surgical intervention
Surgical treatment for septic arthritis of the ankle joint was performed as follows. The patient was placed in a supine position on the orthopedic table. The surgery was performed under regional or intravenous anesthesia. After the preparation of the surgical site, the synovial fistula was used for staining the area of septic-necrotic foci of the ankle joint with a solution of brilliant green. The anterior approach was used for the exposure of the joint. This incision exposes the tibiofibular syndesmosis, the anterior surface of the fibular, the neck of the talus, and the articular cavity of the ankle joint. If the synovial fistula was located in the projection of the incision, it was dissected during the joint exposure. If the synovial fistula was located outside the projection of the incision, it was dissected with a separate incision to the depth of the soft tissue damage. After the exposure of the joint cavity, surgical treatment of the septic-necrotic focus was performed with necrosequestrectomy and resection of the tibia and astragalus within the area of healthy tissue. Further, the Ilizarov apparatus with three external supports was mounted. Figure 1 shows the layout of the surgical techniques. For the formation of proximal basic support of the external fixation via the distal metaepiphyses of the tibia and astragalus, two pins (1) were installed crosswise and fixed in the first ring frame. A percutaneous pin (2) was inserted via the diaphysis of the tibia and fixed on the second ring frame. For the formation of the distal basic support of the external fixation, pins with support plates (3) were inserted via the calcaneal and metatarsal bones towards each other and fixed on the third ring support. By the distraction in the area of resection of the tibia and astragalus, a cavity in the ankle joint was created. Via this cavity, additional punctures were made in the projection of lateral and medial malleolus. A perforated polyvinyl chloride tube (4) was placed in the soft tissues and fixed it on the skin with loop sutures. Bonesaw-lines of the tibia and astragalus were brought closer to each other to fit the size of the drainage tube (Figure 1).
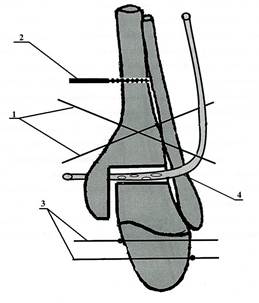
Figure 1. The layout of the surgical technique for the treatment of septic arthritis of the ankle joint
The wound was closed with loot sutures. The sanitation of the created cavity via the drainage tube was performed with antiseptic solutions for 10-15 minutes on the operating table. The volume of the liquid was up to 1-2 L. Antibacterial therapy was performed for 7-10 after the surgery. The choice of drugs depended on the results obtained from the bacteriological study of the sensitivity of pathogenic microorganisms to antibiotics. In the post-operative period, sanitation of septic-necrotic focus was performed by constant draining of the formed cavity with antiseptic solutions for 10-14 days. The lavage of the cavity was performed with a 0.5% water solution of chlorhexidine or 5% water solution of argovit. Twice a day, the drainage tube was closed and a 10% solution of betadine or a solution of antibiotic was injected into the cavity for 20-30 minutes. Every 3rd day, bacteriological control was performed by the bacteriological study of the lavage liquid. When sterile culture was obtained three times, the perforated tube was removed. After the removal of a drainage tube, tibia and astragalus were gradually drawn together in the apparatus of external fixation. The external fixation was switched to the mode of stabilization with the damaged limb support. The fixation in the apparatus continued to the formation of the radiological picture of the bone ankyloses in the ankle joint. Indications for the removal of the transcutaneous fixation are radiological features of the formation of the osteal block, lack of mobility in the joint, and pains during the clinical probe. The time of the apparatus removal was defined individually depending on the radiological dynamics of the formation of osteal regenerate [5].
RESULTS.
The proposed technology of the treatment of septic osteoarthritis in the ankle joint was used in 22 patients. In all the cases, a stable remission of the inflammatory process and formation of the bone ankyloses in the ankle joint was observed.
Patients’ hospitalization for long-term treatment of septic-necrotic focus was 14-16 days. Two days after the surgery, the patients were mobile and self-sufficient in movements and care. After the removal of the drainage and compression in the external fixation, the patients were allowed to walk with a moderate load on the operated limb using crutches.
The time of fixation varied from 16 to 20 weeks. When the external fixation was removed, the patients had to use crutches for 4 more weeks constantly increasing the load on the operated limb. By the end of the month, the limb supporting function completely restored.
The economic effectiveness of the technology is based on the lack of recurrence of the inflammation of the ankle joint for 5 years that does not require repeated inpatient treatment.
During the treatment, two patients had marginal necrosis in the area of the post-operative wound, which was associated with the deficit of soft tissues involved in the inflammatory process that healed with secondary retention. In three cases, superficial inflammation of soft tissues in the area of the inserted pins was registered. These complications were prevented by a rational choice of perosseous elements or titan pins with bioceramic covering [6].
To illustrate the proposed method, a clinical case of a long-term recurring inflammation process in the ankle joint developed as a complication after an open malleolus fracture is presented.
Patient A. aged 43 years old was admitted to the hospital with the diagnosis: recrudescence of chronic osteomyelitis of the distal metaepiphysis of the left tibia. Fistulous form.
Earlier, the patients had several surgeries for chronic osteomyelitis of the left malleolus and foot at the local hospital. The treatment resulted in the formation of the ankyloses of the foot arch joints and anterior part of the foot, which is presented in Figures. The patient underwent arthrotomy of the ankle joint with the dissection of the fistula. After the removal of necrotic tissues, the resection of articular surfaces of the astragalus and tibia was performed in the area of healthy bone tissue. A three-support external fixation was installed on the left lower leg and foot. The distraction was provided and a perforated drainage tube was inserted in the ankle joint cavity (Figure 2A) (the drainage tube is marked with an arrow). Two weeks after the period when the sterile culture was obtained three times, the drainage tube was removed. A compression of bonesaw-lines of the astragalus and tibia was performed (Figure 2B).
 A
A 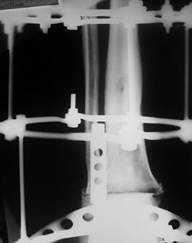 B
B
Figure 2. X-ray imaging of the joint ankle of Patient A.: A – after the installation of the drainage tube in the joint cavity; B – after the removal of the drainage and compression of bonesaw-line of the astragal and tibia.
Three and a half months after the treatment, the control X-ray image revealed a formation of osteal ankyloses in the area of articular surfaces of the astragalus and tibia (Figure 3).

Figure 3. X-ray imaging of the ankle joint of patient A. in 5 months after the surgery
The external fixation was removed. The patient was adapted to walking with crutches with a constant increase in the load on the left foot. Five months after the treatment, the patient started to move without additional support. Pain syndrome resolved. No recurrence of the inflammation was registered for 5 years.
CONCLUSIONS.
The proposed method of treatment of septic arthritis of the ankle joint proved its effectiveness in the clinical practice. The treatment provided a 5-year and more period free of recurrence in patients who were treated for inflammation. The method provides the resolution of the inflammation due to the formation of optimum conditions for the sanitation of the septic foci by the creation of an artificial joint cavity. It also provides optimum conditions for the formation of bone ankylosis in the area of the ankle joint by means of controlled compression in the external fixation. It should be noted that the use of the proposed method in clinical practice does not require additional expenses. It is performed with standard parts of the apparatus of external fixation and available medical consumables. High clinical effectiveness, simplicity, and availability of the proposed method allow the authors to recommend it not only in specialized scientific research institutes but also by traumatologists in the municipal, oblast, regional, and republic hospitals.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
The authors declare no conflict of interest
Библиографическая ссылка
Grazhdanov K.A., Barabash A.P., Barabash Yu.A., Kauts O.A., Zuev P.P. METHOD OF TREATMENT OF PURULENT ARTHRITIS OF THE ANKLE // Современные проблемы науки и образования. Хирургия. 2018. № 3. С. 27-31;URL: https://clinical-medicine.ru/ru/article/view?id=16 (дата обращения: 04.04.2025).
DOI: https://doi.org/10.17513/mpses.16