


Aims
The work was aimed at morphological substantiation of choosing tracheotracheal anastomosis at varying extent of resection.
Materials and methods
The work presents data of morphological changes in the tracheal wall tissues in the anastomosis region in resection of various extents. For this purpose, a chronic experiment was conducted in animals (54 dogs), which simulated clinical cases of treatment of patients with tracheal pathology. The morphology of cartilagenous tissue, perichondrium and surrounding loose connective tissue was assessed. The cellular composition of tissues in the region of anastomosis was studied.
Results
The study showed direct relation between pathological changes in the region of tracheotracheal anastomosis and extent of resection. When more than four tracheal rings were resected, significant impairment of architectonics of cartilagenous tissue and perichondrium was revealed, up to necrosis, which leads to tracheomalacia and increased risk of stenotic process. Slowing of reparative processes and the presence of chronic, slow-current inflammatory process in the region of anastomosis were noted, which is due to the anatomical features of the organ blood supply.
Conclusions
The analysis of the obtained morphological data suggests inadmissibility of continuous suture on the trachea when making tracheal anastomosis, and feasibility of Davydov’s suture and the proposed technique.

- Dydykin S.S. Anatomical-experimental justification for allograft of trachea on vascular pedicle: monograph [Anatomo-eksperimental'noe obosnovanie allotransplantatsii trakhei na sosudistoi nozhke: monografiia]. Moscow, KDU, 2006, 112 p.
- Mishina E.S., Zatolokina M.A., Netiaga A.A. et al. Reactive changes of connective tissue anterior abdominal wall in the early postoperative period with using experimental samples net endoprosthesis antibacterial coating [Reaktivnye izmeneniia soedinitel'noi tkani perednei briushnoi stenki v rannem posleoperatsionnom periode pri ispol'zovanii opytnykh obraztsov setchatykh endoprotezov s antibakterial'nym pokrytiem]. Modern problems of science and education - Sovremennye problemy nauki i obrazovaniia, 2015, vol. 1, no. 2, available at: https://www.science-education.ru/en/article/view?id=18056. (accessed 13.11.2017).
- Parshin V.D., Volkov A.A., Parshin V.V. Tracheoplasty after circular trachea resection [Shov posle tsirkuliarnoi rezektsii trakhei]. Pirogov Russian Journal of Surgery - Khirurgiya. Zhurnal imeni N.I. Pirogova, 2011, no. 12, pp. 4-9.
- Bystrenin A.V. To assess the results of surgical treatment to restore larynx and trachea lumen in case of their chronic stenosis [K otsenke rezul'tatov khirurgicheskogo lecheniia po vosstanovleniiu prosveta gortani i trakhei pri ikh khronicheskikh stenozakh]. Bulletin of otorhinolaryngology - Vestnik otorinolaringologii, 2010, no. 6, pp. 27-28.
- Kichigina O.S., Egorova E.O., Bezhin A.I. Method of forming tracheotracheal anastomosis in circular trachea incisions: Patent 2456931 of Russian Federation [Sposob formirovaniia trakheotrakheal'nogo anastomoza pri tsirkuliarnykh razrezakh trakhei: Pat. 2456931 Rossiiskaia Federatsiia], № 2011113843/14, Kursk, Kursk State Medical University, 2012.
INTRODUCTION
Successful surgery depends on a profound knowledge of the surgical anatomy of the operational area and the surgeon’s experience. Thus, the outcome of the surgery on the trachea depends on the place of tracheo-tracheal anastomosis. The blood supply of the organ is exerted via the capillary net of the membrane part that is poorly developed in the upper and midthoracic sections. These anatomically weak spots can increase the risk of the development of post-operational complications in the areas of anastomosis [1]. The trachea primarily consists of cartilaginous tissue. Its blood supply is performed due to the perichondrium via diffusion. Thus, the damage of the perichondrium leads to cartilage destruction and its substitution with connective tissue [2].
The specified anatomical facts indicate that the trachea is a surgically complicated organ [3]. Thus, a detailed histological study on the tracheal anastomosis, especially, in the conditions of tension, will allow specialists to improve the suturing outcome, which is an acute issue in modern thoracic surgery [4].
MATERIALS AND METHODS
The study included three methods of formation of tracheo-tracheal anastomosis: continuous suture, Davydov’s suture, and the method proposed by the authors [5].
The study was designed as a long-term experiment that included 54 outbred dogs. To make the experiment closer to the clinical situation (repeated surgery in patients with tracheal stenosis), the study was divided into several stages (Table 1).
The study was performed according to all the regulations, protocols, and ethical norms on the studies with experimental animals (Strasburg, France, 1986, the decree of the MH RF No. 267 dated June 19, 2003).
At the next stage, the degree of tracheal stenosis lumen was evaluated in the area of tracheo-tracheal anastomosis by the classification of Freitag at el. (2007), where stage I – 25%, stage II – 26-50%, stage III – 51-75%, stage IV – 76-90%, stage V – 91-100%.
The histological study included 1.5 x 1.5 cm samples of the trachea taken from the area of anastomosis. Histological sections were made from the blocks of samples and van Gieson hematoxylin and eosin-stained.
The histological and morphometrical study was performed at x200 and x400 magnification. It included the evaluation of cartilaginous tissue, perichondrium, surrounding loose connective tissue, and the cellular composition count in the area of anastomosis.
For the objectivization of the processes observed in tissues, the authors used the cellular index, i.e. the ratio of resident cells (macrophages, fibroblasts, fibrocytes) to non-resident cells (neutrophils, lymphocytes, eosinophils).
It was suggested that the cellular index < 1 indicates the exudative phase of the inflammatory process and the cellular index > 1 indicates the proliferative phase.
Table 1. Distribution of experimental animals by the series, dates, and volume of tracheal resection in the conditions of the chronic experiment
RESULTS
The experiment “without tension” showed that the method of tracheo-tracheal anastomosis with suturing of the organ without its resection was not significant because, in this study, the stenosing of the tracheal lumen was not observed.
In the experiment with the resection of 4 tracheal rings in the 3rd series of tests on Day 7 and Day 30, the area of stenosis was 5 and 2.5 times smaller, respectively, in comparison with the 1st and 2nd series of tests.
In the experiment with the resection of 8 tracheal rings in the 3rd series of tests, the area of stenosis was 2.5 and 2 times smaller in comparison with the 1st and 2nd series, respectively.
The histological study in the experiment “without tension” in the 1st and 2nd series of tests revealed inflammatory events observed during the experiment. At later stages, necrosis was observed (Figure 1).
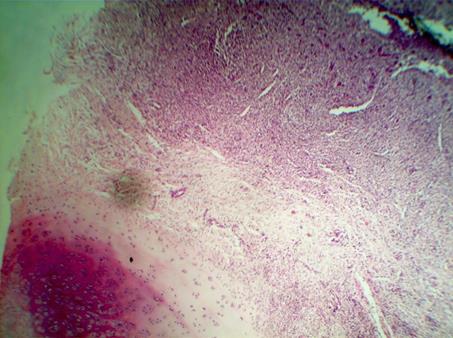
Figure 1. Photomicrography of the area of anastomosis in the 1st series of tests on Day 30. Inflammatory cellular infiltrate with the foci of necrosis. Hematoxylin and eosin staining. Magnification x200.
The 3rd series of tests showed a regular change in the stages of aseptic inflammation. By Day 30, there was a formation of a dense connective-tissue cicatrix.
The analysis of the morphometric picture showed that at the early stages, in the conditions “without tensioning”, there was an exudative phase of the inflammatory process observed in all 3 series of tests.
On day 14, in the 1st and 2nd series of tests, the cellular component prevailed over the fibrous one, which indicated the continued inflammation. However, in the 3rd series of tests, the count of globocellular formed elements and fibrocytes became equal, which indicated reparative processes.
On Day 30, in the 1st and 2nd series of tests, the morphometrical picture barely changed in comparison with Day 14, and in the 3rd series, the formation of the connective tissue cicatrix was registered (more than 50% of cells were represented by fibroblasts).
Thus, in the group “without tension”, only in the 3rd series of tests by Day 30, a formed connective tissue cicatrix was registered, while in the 1st and 2nd series of tests at this stage, the reparative process just began.
The morphological picture of the samples of the trachea in the area of anastomosis after the “resection of 4 tracheal rings” significantly differed. In the 1st series of tests, destructive changes were expressed in the area of the perichondrium. In the 2nd and 3rd series of tests, there were changes in the mucosal and submucosal layers of the trachea. Inflammatory changes were not registered (Figure 2). In the area of anastomosis, the formation of the connective tissue capsule was observed.
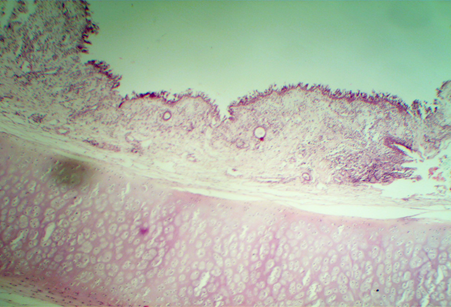
Figure 2. Photomicrography of the area of anastomosis in the 3rd series of tests on Day 30. Metaplasia of the ciliated epithelium in the trachea. Heterofunctional desquamation.
Hematoxylin and eosin staining. Magnification x200.
On Day 7, after the “resection of 4 tracheal rings”, an inflammatory process was observed in the area of anastomoses in all the series of tests. The number of leucocyte cells was around 75%, fibroblast cells – 20-30%.
On Day 14, the morphometric picture did not change in comparison with Day 7.
By Day 30, in the 2nd and 3rd series of tests, there was a tendency towards the change of phases of the regeneration process. Thus, there were 50% of leukocyte cells and 40% of fibroblastic cells. In the 1st series of tests, the morphometric picture did not change in comparison with the previous period.
Thus, after the “resection of 4 tracheal rings”, a continuous inflammatory process was observed that started to resolve by Day 30 and only in the 2nd and 3rd series of tests.
In the group with the “resection of 8 tracheal rings”, in the 1st series of tests, the authors observed the damage of tissues with sutures in the area of anastomosis, development of septic inflammation that did not resolve by the later stages. Expressed areas of necrosis of the perichondrium that affected the cartilage were observed (Figure 3).
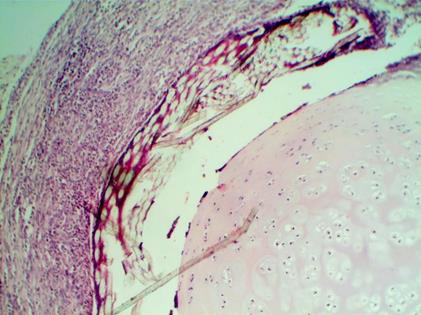
Figure 3. Photomicrography of the area of anastomosis in the 1st series of tests on Day 30. Destruction of perichondrium and cartilage. Hematoxylin and eosin staining. Magnification x200.
In the 2nd series of tests, by Day 14, the authors observed the transition from the phase of exudation to the phase of proliferation but, by Day 30, there were no significant changes revealed. Vacuolization of chondrocytes, shrinkage of nuclei, and disturbance of zonality of cartilaginous tissue were observed (Figure 4). In the area adjoining the perichondrium, there was significant infiltration due to the improvement of blood supply, which was confirmed by an increase in the number of vessels per section area.
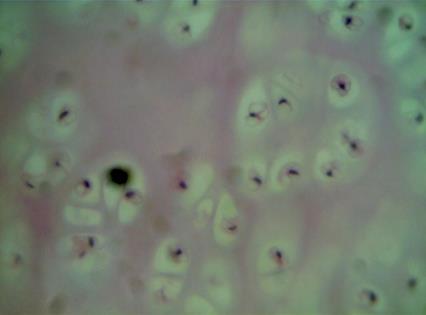
Figure 4. Photomicrography of the area of anastomosis in the 2nd series of tests on Day 30. Changes in isogenic groups, shrinkage of chondrocyte nuclei. Hematoxylin and eosin staining. Magnification x400.
In the 3rd series of tests, there were necrotic changes in the mucosal layer, focal thickening of the epithelium, crateriform dilatation of submucosal glands. Blood filling and stasis of blood vessels were observed. The formation of immature connective tissue cicatrix was registered, which led to a continuous transformation of the connective tissue capsule around the anastomosis (Figure 5).
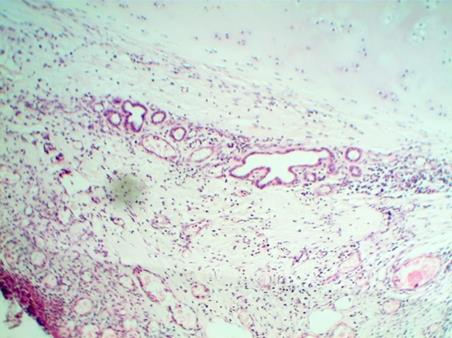
Figure 5. Photomicrography of the mucosa and submucosal layer in the area of anastomosis in the 3rd series of tests on Day 30. Hematoxylin and eosin staining. Magnification x200.
On Day 7, the morphological analysis of samples after the “resection of 8 tracheal rings” in all the studied series showed a similar morphological picture with the samples after the “resection of 4 tracheal rings”.
On Day 14 and Day 30, in the 2nd and 3rd series of tests after the “resection of 8 tracheal rings”, there was a tendency towards the transition from the phase of exudation to the phase of proliferation (the cellular index was approaching 1). At this stage, in the 1st series of tests, there was a significant inflammatory reaction (the cellular index was significantly lower than 1).
Thus, after the “resection of 8 tracheal rings” in all the studied series at all the stages, there was an inflammatory process in the area of tracheo-tracheal anastomosis. However, only in the 2nd and 3rd series of tests, there was a tendency towards the reduction of inflammatory events.
CONCLUSIONS
The formation of tracheo-tracheal anastomosis after the resection of more than 4 tracheal rings is associated with high post-operational risks.
It is not advisable to apply continuous suturing during the formation of tracheo-tracheal anastomosis with tension.
The proposed method of trachea suturing is performed considering anatomo-histological peculiarities of the organ, which contributes to the improvement of regenerative processes in the area of anastomosis.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
The authors declare no conflict of interest
SUPPLEMENTARY DATA (DOI).
Библиографическая ссылка
Kichigina O.S., Zatolokina M.A., Mishina E.S., Nikulin A.I. MORPHOLOGICAL REASONS FOR CHOOSING TRACHEOTRACHEAL ANASTOMOSIS AT VARYING RESECTION EXTENT // Современные проблемы науки и образования. Хирургия. 2018. № 1. С. 9-14;URL: https://clinical-medicine.ru/ru/article/view?id=9 (дата обращения: 04.04.2025).
DOI: https://doi.org/10.17513/mpses.9